Bracing
The three dimensional scoliosis brace complements the Schroth exercises performed by the patient, placing their spine in a similar over-corrected position. This overcorrection unloads the apical vertebrae of the curve allowing symmetrical growth to occur. As with the Schroth method we are focusing on reversing the vicious cycle of asymmetrical loading. Research indicates this asymmetrical loading reduces the growth rate of the bone.1 By unloading or reducing the load placed on the wedged vertebrae we increase the growth rate of the affected vertebrae(s). This is known as the Heuter-Volkmann principle.
Current asymmetrical (3 dimensional braces) braces provide larger in-brace correction than symmetrical braces.2 Our brace is designed via CAD/CAM (Computer Aided Design/Computer Aided Manufacturing), these methods are proven to provide better in-brace correction than plaster moulded braces.4 Our 3 dimensional brace uses a classification based method, which is superior to some of the new braces that are made by CAD/CAM design with no applied classification system.2
Bracing is normally indicated in patients that have curves greater than 25 degrees and have some growth remaining.5 Bracing at this stage can reduce the likelihood of progression to surgical levels6,7,8 which is generally indicated with curves above 50 degrees. The more compliant a patient is with wearing the brace the better the final outcome.6
Weistein et al also showed that patients that were assigned to wearing a brace, 75% had curves that didn’t progress to surgical indicated levels (50 degrees), the group that didn’t wear a brace only 42% didn’t progress to 50 degrees.6 Compliance of wearing the brace is very important. Patients who wore the brace for less than 6 hours a day had roughly the same success rate as those patients who did not wear the brace at all. Those who wore the brace more than 13+ hours a day had a success rate of 90% or higher.6
Vicious Cycle vs Virtuous Cycle
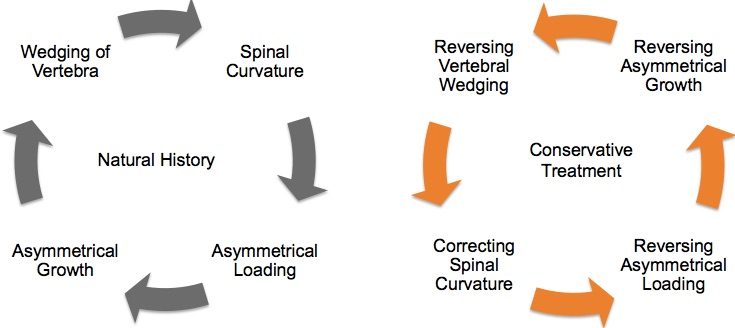
The aim of the Schroth Method and/or bracing in a growing spine is to reverse the asymmetrical loading, hence reversing the asymmetrical growth, reverse the wedging and improving spinal curvature.
Combining bracing with scoliosis specific exercises such as the Schroth Method has shown to be more effective than treatment or bracing alone.2 The longer a patient is in their specific spinal overcorrected position, the better the outcome.3
The Bracing Process
At Victoria Sports and Rehabilitation Clinic we manage the bracing process from start to finish. This includes the design, manufacturing, fitting and modifications of the brace, working directly with Dr Hans-Rudolf Weiss and experienced scoliosis Orthotist – Nick Muller from Peninsula Orthotics. Each brace is customised to the individual’s curve and measurements and we are able to create the brace and fit it to the patient in as little as 2 days, due to our manufacturing being based in Australia. The fitting process is outlined below:
- Initial Brace Fitting (90 Min appointment)
- 1 week In-Brace EOS Xray (or timeframe as instructed by referring specialist)
- 1 week Brace Follow-up and modifications as required (60 Min appointment)
- 6 week Brace Follow-up (60 Min appointment)
- 3 month Out of Brace EOS Xray
- 3 month Brace Follow-up (60 Min appointment)
- Ongoing 3 monthly review
1 – Akel I, Yazici M. The management of growing spine deformities. J Child Orthop. 2009 Feb
2 -Weiss HR, Kleban A. Development of CAD/CAM Based Brace Models for the Treatment of Patients with Scoliosis-Classification Based Approach versus Finite Element Modelling. Asian Spine J. 2015 Oct 9
3 – Weiss HR. Standardising the treatment with Chêneau braces via CAD: Prospects and risks. OA Musculoskeletal Medicine. 2014 May 03
4 – Sankar W, Albrektson J, Lerman L, Tolo VT, Skaggs DL. Scoliosis in-brace curve correction and patient preference of CAD/CAM versus plaster moulded TLSOs. J Child Orthop. 2007 Dec
5 – Negrini S, Aulisa A, Aulisa L, Circo A, de Mauroy JC, Durmala J, Grivas T, Knott P, Kotwicki T, Maruyama T, Minozzi S, O’Brien J, Papadopoulos D, Rigo M, Rivard C, Romano M, Wynne J, Villagrasa M, Weiss HR, Zaina F. 2011 SOSORT guidelines: Orthopaedic and Rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis 2012
6 – Stuart L. Weinstein, M.D., Lori A. Dolan, Ph.D., James G. Wright, M.D., M.P.H., and Matthew B. Dobbs, M.D. Effects of Bracing in Adolescents with Idiopathic Scoliosis. N Engl J Med 2013
7 – De Giorgi S, Piazzolla A, Tafuri S, Borracci C, Martucci A, De Giorgi G. Cheneau brace for adolescent idiopathic scoliosis: long-term results. Can it prevent surgery? European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2013
8 – Nachemson A, Peterson L. Effectiveness of treatment with a brace in girls who have adolescent idiopathic scoliosis. A prospective, controlled study based on data from the Brace Study of the Scoliosis Research Society. J Bone Joint Surg Am. 1995
9 – Negrini S, Donzelli S, Lusini M, Minnella S, Zaina F. The effectiveness of combined bracing and exercise in adolescent idiopathic scoliosis based on SRS and SOSORT criteria: a prospective study. BMC Musculoskelet Disord. 2014.